

Chronic Pain:
Living with chronic pain can be exhausting—physically, emotionally, and psychologically. Our chronic pain therapy is grounded in a trauma- and nervous-system–informed understanding of how pain is created, maintained, and healed. Our work centres on EMDR (Eye Movement Desensitization and Reprocessing), supported by parts work, pain reprocessing theory, and polyvagal theory, to address both pain and the emotional distress that often accompanies it.
*Below, I have outlined the research in layman's terms. Please find the scientific explanation at the bottom of this page and in the attached research studies.
Bucket Metaphor for Chronic Pain and Illness
Every individual’s nervous system and ability to tolerate stress can be seen as a bucket filled with water. If your life is less stressful, or you have strong distress tolerance, adaptability, and good heart rate variability, you will tend to have less water in your bucket. Therefore, your nervous system can handle a lot of stress, both physical trauma (e.g., a rear-ending) and emotional trauma, before your bucket overflows and your nervous system becomes sensitized. In other words, you have a larger buffer zone for the development of central sensitization (CS) and chronic pain. On the other hand, if you have had a lot of stressors in your life, your bucket will tend to be more full and more easily susceptible to overflow leading to central sensitization. When you have a nervous system that is sensitized, this can strengthen pain pathways between the brain and nerves, and amplify pain signals, leading to chronic pain.
Studies have shown that if you have experienced trauma, your bucket can almost always be nearly full, even decades later. This is why chronic pain is reported by 25% to 93% of patients with PTSD, which is 2 to 5 times the rate of chronic pain in the general population. In addition, high rates of PTSD ranging between 22% and 49% are found among patients with chronic pain, which is 2 to 4 times the rate of PTSD in the general population. Although chronic pain and PTSD can each have a profound impact on individuals' health and quality of life, the coexistence of both conditions is even more destructive and devastating (Defrin et al., 2015). In addition to childhood stress and trauma, factors like financial stressors, child care stressors, perfectionism, and especially, a highly stressful job also lead to a nearly full bucket (i.e., your nervous system will be more sensitized). When your bucket is almost full, seemingly "minor" incidents/injuries that adaptable nervous systems can heal from, like a rear-ending or lifting a heavy box, overflows a person with CS's bucket. This can lead to a hyperactive nervous system that interprets these stressors as hyper-dangerous and locks that pain in the brain and body, potentially for years/decades, even though the original injury has healed.
Central sensitization is often shaped by:
Physical injury or chronic illness
Medical or developmental trauma
Chronic stress or emotional overwhelm
Anxiety, depression, grief, or feelings of helplessness
Moreover, chronic pain/illness itself is traumatic and can lead to issues like depression and anxiety, which further stresses the nervous system and keeps one’s bucket full. In turn, a feedback loop for the pain is created – as the pain causes stress, the stress keeps your bucket full, which then exacerbates the pain, which causes additional stress, and so on. In addition, the longer the brain amplifies those pain pathways as time goes on, the association becomes stronger by “clearing the pathway”, making it easier to for the brain to send false pain signals and exacerbate pain. Moreover, many people who suffer from chronic pain and illness aren’t believed, are misdiagnosed, and/or experience medical trauma throughout their journey of pain management. This also fills one’s bucket and reinforces the feedback loop of pain. Because pain is processed in the brain, emotional and relational experiences play a significant role in how pain is felt. Effective chronic pain treatment therefore needs to address the nervous system, emotional memory, and meaning-making, not just the traditional medical model approach of treating physical symptoms/tissue damage (Bussières et al,, 2023).
Integrating Parts Work and Somatic Approaches
Chronic pain often involves protective parts of the nervous system that developed to keep you safe. Parts work (IFS-informed) helps identify and gently work with these protective responses—such as hypervigilance, shutdown, or over-efforting—without forcing change.
Somatic and polyvagal-informed approaches are integrated alongside EMDR to:
Support nervous system regulation and safety
Increase tolerance for body sensations
Reduce fear of pain flares
Restore trust in the Self and body
Together, these approaches help clients build resilience, regulate stress responses, and develop a more compassionate relationship with their bodies.
A Whole-Person Approach to Pain
Chronic pain rarely exists in isolation. It often coexists with anxiety, depression, trauma, and grief. Counselling provides a space to address the full impact of pain—physically, emotionally, and relationally—while supporting meaningful, sustainable change.
Online Counselling for Chronic Pain
As someone who endured both chronic pain and chronic illness for over a decade, I am intimately aware of how pain and illness can make travel and scheduling difficult. Therefore, I offer secure online EMDR or talk therapy from the comfort of your home. This allows you to receive care from a space that feels safe and supportive, without added physical strain, with the flexibility to take breaks or use your pain management tools whenever you'd like throughout the session.
Benefits of online chronic pain counselling include:
Reduced energy expenditure and physical stress
Consistent support during flare-ups
Flexible scheduling aligned with your capacity
Trauma-informed, evidence-based care from home






Understanding Chronic Pain Through the Nervous System
In many cases, chronic pain is not caused by ongoing tissue damage, but by central/neurosomatic sensitization. This occurs when the nervous system becomes overprotective following injury, chronic illness, trauma (both childhood and physical trauma, like a car accident), or prolonged stress. The brain and spinal cord begin to amplify pain signals, interpreting normal or mild sensations as dangerous. Even after the original injury has healed, the nervous system can remain stuck in a state of high alert. Studies have shown that chronic pain and symptoms such as back pain, neck pain, fibromyalgia, pelvic pain, migraines, headaches, fatigue, IBS, dizziness, tinnitus, among many others are often not structurally caused, but occur in the brain due to learned neural pathways.
Chronic Autoimmune Illnesses:
Increasing evidence suggests a link between posttraumatic stress disorder and physical health. Specifically, stress disorders may lead to impairment of the immune system and subsequent autoimmune disease. Individuals who have experienced trauma remain in a perpetual state of hyperarousal/hypervigilance and fear. As such, PTSD is associated with immune, hormonal, and neurobiological abnormalities. Posttraumatic stress has been shown to impede functioning of the hypothalamic pituitary adrenal (HPA) axis, the immune system, and the autonomic nervous system. Furthermore, interactions within the neuro-endocrine system are bidirectional, meaning that hyperarousal and subsequent increased hormonal activity in the nervous system can trigger the release of high levels of stress hormones that further contribute to chronic immune dysregulation and the potential to develop autoimmune disease (Bookwalter et al., 2020; Song Huan et al., 2018).
HOW EMDR CAN HELP CHRONIC PAIN & ILLNESS
How EMDR Supports Chronic Pain & Illness Healing
EMDR is a powerful, evidence-based therapy that helps the brain reprocess distressing memories, sensations, and beliefs that keep the nervous system in a threatened state. In the context of chronic pain, EMDR can directly target both pain pathways and the emotional experiences that reinforce them.
Through EMDR, clients may experience:
Reduction or elimination of pain by calming sensitized neural pathways
Processing of medical trauma, injury, illness, or invasive procedures
Decreased anxiety and fear related to pain sensations
Relief from depression, grief, and identity loss linked to chronic pain
Shifts in deeply held beliefs such as “My body is broken”, “I’m not safe”, or "I am powerless"
By working with how pain is stored and interpreted in the nervous system, EMDR supports integrated healing across mind and body (Grant & Threlfo, 2002; Singla et al., 2025).
Bookwalter, D. B., Roenfeldt, K. A., LeardMann, C. A., Kong, S. Y., Riddle, M. S., & Rull, R. P. (2020). Posttraumatic stress disorder and risk of selected autoimmune diseases among US military personnel. BMC psychiatry, 20(1), 23. https://doi.org/10.1186/s12888-020-2432-9
Conclusion: Active duty military personnel with PTSD may have an elevated risk of a range of autoimmune diseases, regardless of combat experience or prior trauma. Future research is needed to understand potential mechanisms which may inform future mitigative strategies in reducing extra-neuropsychiatric health problems among those with PTSD.
Bussières, A., Hancock, M. J., Elklit, A., Ferreira, M. L., Ferreira, P. H., Stone, L. S., Wideman, T. H., Boruff, J. T., Al Zoubi, F., Chaudhry, F., Tolentino, R., & Hartvigsen, J. (2023). Adverse childhood experience is associated with an increased risk of reporting chronic pain in adulthood: A systematic review and meta-analysis. European Journal of Psychotraumatology, 14(2), 2284025. https://doi.org/10.1080/20008066.2023.2284025
Conclusion: Single and cumulative ACEs are significantly associated with reporting of chronic pain and pain-related disability as an adult.
Deferin, R, Schreiber, S., & Ginzburg, K. (2015). Paradoxical pain perception in posttraumatic stress disorder: The unique role of anxiety and dissociation. The Journal of Pain, 16(10), 961-970. http://www.sciencedirect.com/science/article/pii/S1526590015007579
Conclusion: The paradoxical facets of PTSD and their particular influences over pain perception seem to reinforce the coexistence of PTSD and chronic pain, and should be considered when treating traumatized individuals.
Grant, M., & Threlfo, C. (2002). EMDR in the treatment of chronic pain. Journal of Clinical Psychology, 58(12), 1505–1520. https://doi.org/10.1002/jclp.10101
Conclusion: All clients reported substantially decreased pain levels, decreased negative affect, and increased ability to control their pain following treatment. These results indicate that EMDR may be efficacious in the treatment of chronic pain and that further research is warranted.
Pabón Moreno, A., Gonzalez Galindo, V., Hurtado-Ortiz, A., Licht-Ardila, M., Manrique-Hernández, E. F., Mendoza-Monsalve, A., Pérez-Cárdenas, A. T., Forero, X. J., Portilla, A. J., Silva Sieger, F., & Llanez Anaya, E. (2025). Adverse childhood experiences and their impact on primary headache patients: a cross-sectional study. Frontiers in psychiatry, 16, 1676559. https://doi.org/10.3389/fpsyt.2025.1676559
Conclusion: This study demonstrates a strong relationship between adverse childhood experiences and primary headaches, highlighting the need to incorporate childhood trauma assessment into neurological practice.
Singla, A., Futela, P., Arora, K., Toussaint, L., Ahmad, Z., Murawska Baptista, A., Anstine, C. V., Hurt, R. T., Philpot, L. M., & Mohabbat, A. B. (2025). Eye movement desensitization and reprocessing for chronic pain: A systematic review. Journal of Integrative and Complementary Medicine, 31(12), 1045–1055. https://doi.org/10.1177/27683605251362035
Conclusion: EMDR shows promise for managing chronic pain and addressing associated mental health symptoms. Despite study differences and limitations, the findings of this systematic review support the potential use of EMDR for chronic pain management.
Song Huan, Fang Fang, Tomasson Gunnar, Arnberg Filip K., Mataix-Cols David, Fernández de la Cruz Lorena, Almqvist Catarina, Fall Katja, Valdimarsdóttir Unnur A. Association of Stress-Related Disorders With Subsequent Autoimmune Disease. JAMA. 2018;319(23):2388. doi: 10.1001/jama.2018.7028.
Conclusion: In this Swedish cohort, exposure to a stress-related disorder was significantly associated with increased risk of subsequent autoimmune disease, compared with matched unexposed individuals and with full siblings. Further studies are needed to better understand the underlying mechanisms.
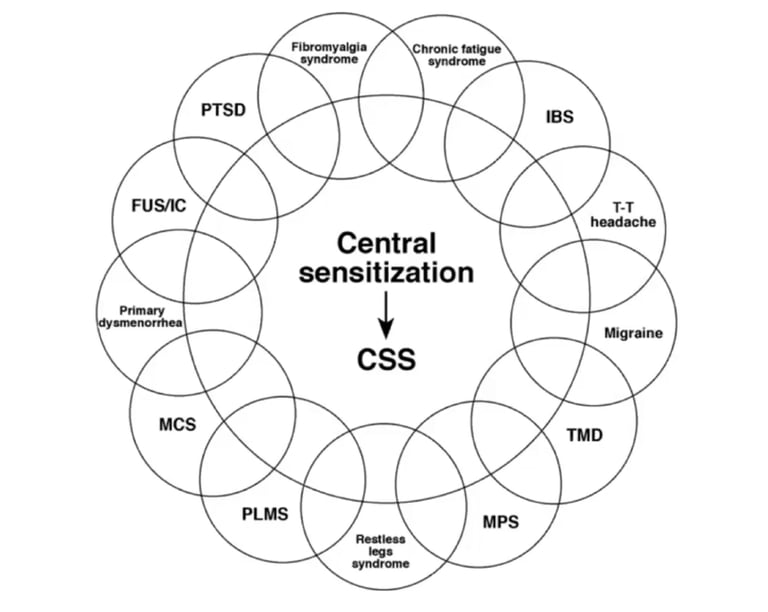
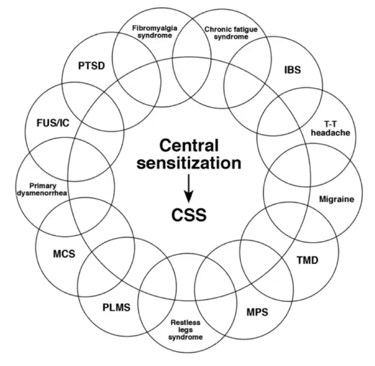
Central Sensitization Explained in Scientific Terms:
Central sensitization (CS) is an elevated responsiveness of nociceptive neurons in the central nervous system (CNS) to their normal or subthreshold peripheral input. The CNS becomes more sensitive to input through functional, structural, and chemical changes. With or without continuing peripheral input, CS may be maintained, and these changes in the nervous system may eventually lead to a persistent, increased state of neuronal reactivity. CS involves an amplification of neural signaling within the CNS that results in pain hypersensitivity. This amplification frequently results in chronic, widespread, and migratory pain, chronic fatigue, sensory hypersensitivity, and many other symptoms. CS is associated with several medical diagnoses, including low back pain, osteoarthritis, whiplash, and fibromyalgia. While, it currently cannot be directly determined clinically; certain symptoms and signs may suggest its presence (Bazancir-Apaydin et al., 2025).
Bazancir-Apaydin, Z., Apaydin, H., Armagan, B., Orhan, K., & Erten, S. (2025). The Role of Central Sensitization in Autoimmune Connective Tissue Diseases: A Comparative Cross-Sectional Study. International journal of rheumatic diseases, 28(1), e70069. https://doi.org/10.1111/1756-185X.70069
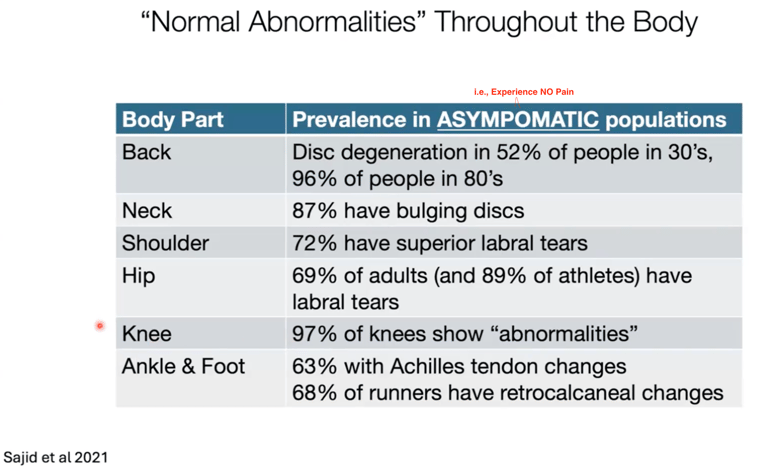
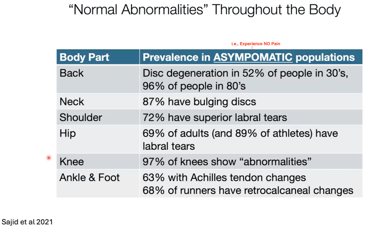
Research on the prevalence of anatomical issues/tissue "damage" as seen on medical imaging where patients have NO chronic pain. Therefore, tissue damage does not always = chronic pain. Change your brain = change the pain.
INTERESTED IN LEARNING MORE?
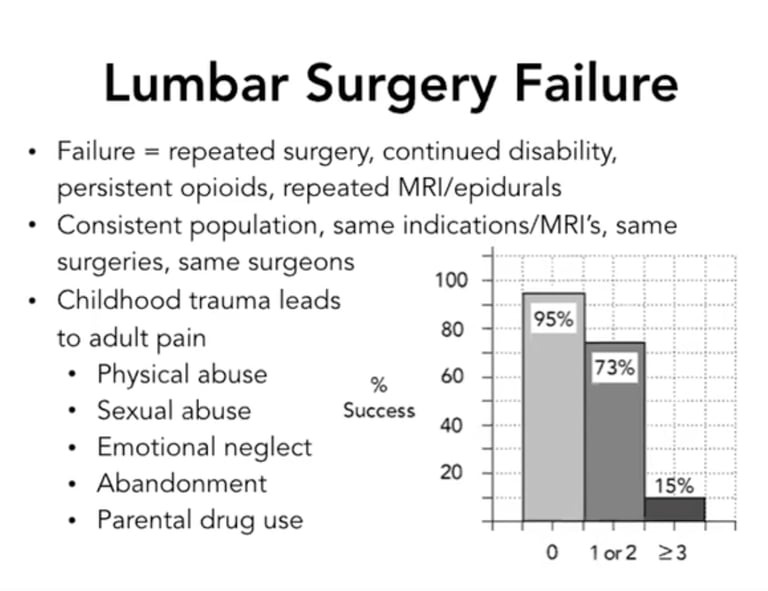
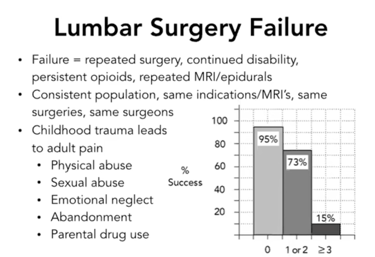
Research indicating that if you had 0 instances of childhood abuse as measured by physical abuse, sexual abuse, emotional neglect, abandonment, or parental drug use, then you have a 95% chance your lumbar surgery will be successful and resolve your chronic low back pain. If you had 1 or 2 instances of those markers of abuse, then you have a 73% chance of successful surgery, and if you had 3 or more markers of abuse, then you have a 15% chance of a successful surgery. Why? Because tissue damage does not always = chronic pain. The pain is often generated from the brain due to a sensitized nervous system (Schofferman et al., 1992).
Since the traditional medical model of "pain = tissue damage" has always been presented to us as chronic pain patients, I have included some research since it can be challenging to wrap your head around this concept of pain generation coming from a sensitized brain.
A very helpful book for chronic pain/illness sufferers!
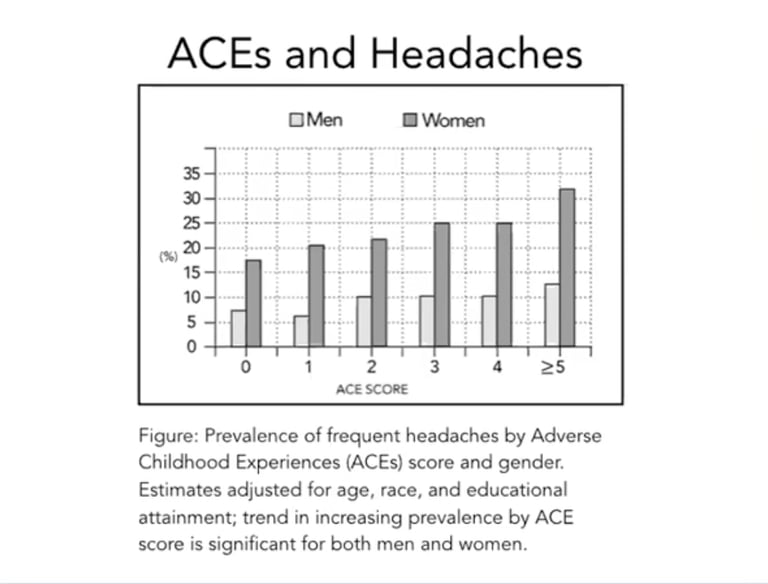
Research on the positive association between the prevalence of chronic headaches and Adverse Childhood Experiences (ACE) scores. While the trend is there for men, women are more greatly impacted, potentially due to higher rates of trauma among women vs. men. Also, see the study by Pabón Moreno et al., 2025 listed below.
CHRONIC PAIN IS REAL
But so is the brain’s capacity to change. EMDR taps into these natural healing abilities of the brain and calms overactive pain signals. With the right support, the nervous system can learn safety again, and meaningful reductions in pain and emotional distress are possible.